Quietly, but steadily India-born Dr V K Raju has created a movement focussing on the urgency of containing the potential diabetes epidemic in India. The International Diabetes Federation estimates that nearly 20 percent of the world’s population with diabetes (61.3 million people) lives in India, and therefore, Dr Raju’s volunteerwork in India takes immense significance.
Although this West Virginia ophthalmologist moved to the US many years ago, he never left his home behind – and he honors his roots with his work. He makes a difference in the lives of thousands of West Virginia residents in his private practice – and thousands more in India when he returns there on his volunteer missions. All his volunteer work in India and elsewhere is done through the nonprofit Eye Foundation of America, which focuses on corrective and preventive medical procedures on eye and outreach in remote areas of the developing world, where there is no medical care or its cost prohibitive. India
remains Dr Raju’s main focus, primarily because diabetes there is increasingly becoming the root cause for preventable blindness.
Dr Raju recently expanded the program of voluntary services to reach 100,000 diabetics in India and in West Virginia.
Quoting a report in the Australian Medical Journal, Dr Raju says, “India currently faces an uncertain future in relation to the potential burden that diabetes may impose upon the country.”
Although the Indian urban population, Dr Raju explained, has access to reliable screening methods and anti-diabeticmedications, such health benefits were not often available to the rural patients. There was a disproportionate allocation of health resources between urban and rural areas, and in addition poverty in rural areas may be multi-faceted, he said. “Food insecurity, illiteracy, poor sanitation, and dominance of communicable diseases may all contribute, which suggests that both policy makers and local governments may be undermining and under-prioritizing the looming threat of diabetes,” he said quoted the Australian Medical Journal.
It is predicted that by 2030 diabetes may afflict up to 79.4 million individuals in India, while China (42.3 million) and the United States (30.3 million) will also see significant increases in those affected by the disease. Obesity, Dr Raju said was one of the major risk factors for diabetes, yet there has been little research focusing on this risk factor across India.
Despite having lower overweight and obesity rates, India has a higher prevalence of diabetes compared to western countries suggesting that diabetes may occur at a much lower body mass index (BMI) in Indians compared with Europeans. Therefore, relatively lean Indian adults with a lower BMI may be at equal risk as those who are obese. Additionally, studies indicate, Indians were genetically predisposed to the development of coronary artery disease due to dyslipidaemia and low levels of high density lipoproteins; these determinants make Indians more prone to development of the complications of diabetes at an early age (20-40 years) compared with Caucasians (>50 years) and indicate that diabetes must be carefully screened and monitored regardless of patient age within India.
To reduce the disease burden that diabetes creates in India, Dr Raju said appropriate government interventions and combined efforts from all the stakeholders of the society were required. Clinicians may be targeted to facilitate the implementation of screening and early detection programs, diabetes prevention, self-management counselling, and therapeutic management of diabetes in accordance with the appropriate local guidelines form the backbone of controlling the predicted diabetes epidemic.
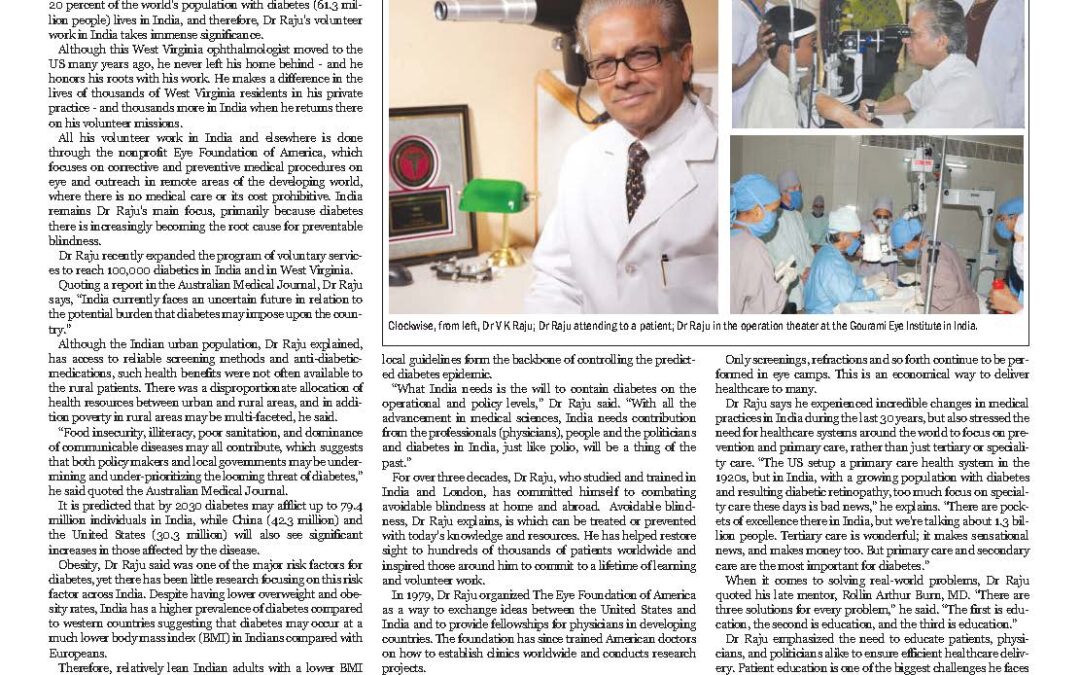
“What India needs is the will to contain diabetes on the operational and policy levels,” Dr Raju said. “With all the advancement in medical sciences, India needs contribution from the professionals (physicians), people and the politicians and diabetes in India, just like polio, will be a thing of the past.” For over three decades, Dr Raju, who studied and trained in India and London, has committed himself to combating avoidable blindness at home and abroad. Avoidable blindness, Dr Raju explains, is which can be treated or prevented with today’s knowledge and resources. He has helped restore sight to hundreds of thousands of patients worldwide and inspired those around him to commit to a lifetime of learning and volunteer work. In 1979, Dr Raju organized The Eye Foundation of America as a way to exchange ideas between the United States and India and to provide fellowships for physicians in developing countries. The foundation has since trained American doctors on how to establish clinics worldwide and conducts research projects. Dr Raju’s humanitarian work began in 1977, shortly after he accepted a faculty position at West Virginia University. “I went on a vacation to India, and a farmer came to show his eyes to me, and I did not have any instruments [to treat him],” he said. The lack of medical care available around his hometown of Rajahmundry prompted Dr Raju to return to India the next year and provide free and subsidized eyecare services to local residents, especially in rural areas.
Two years later, Dr Raju began making annual “eye relief” trips to India, recruiting other doctors and eyecare professionals to come with him. Through these “eye camps,” Dr Raju and his team were able to provide much-needed care to large numbers of patients without the need for them to travel to a hospital- overcoming a major obstacle in the delivery of healthcare in India. Today, all the surgical procedures are performed at Goutami Eye Institute in Andhra Pradesh. Only screenings, refractions and so forth continue to be performed in eye camps. This is an economical way to deliver healthcare to many.
Dr Raju says he experienced incredible changes in medical practices in India during the last 30 years, but also stressed the need for healthcare systems around the world to focus on prevention and primary care, rather than just tertiary or speciality care. “The US setup a primary care health system in the 1920s, but in India, with a growing population with diabetes and resulting diabetic retinopathy, too much focus on specialty care these days is bad news,” he explains. “There are pockets of excellence there in India, but we’re talking about 1.3 billion people. Tertiary care is wonderful; it makes sensational news, and makes money too. But primary care and secondary care are the most important for diabetes.”
When it comes to solving real-world problems, Dr Raju quoted his late mentor, Rollin Arthur Burn, MD. “There are three solutions for every problem,” he said. “The first is education, the second is education, and the third is education.” Dr Raju emphasized the need to educate patients, physicians, and politicians alike to ensure efficient healthcare delivery. Patient education is one of the biggest challenges he faces as an ophthalmologist, both in the US and the developing world.
As a physician, he has worked tirelessly to give patients knowledge that is critical to how they care for their eyes. Dr Raju estimates that the foundation has provided critical care to more than 2 million people globally. Its staff has performed some 300,000 sight-restoring operations to date.
Dr Raju and the Eye Foundation are also working closely with the West Virginia University’s School of Public Health, Monongalia General Hospital and the Rotary International to launch a study on pre-diabetes in the state. The focal point of the program is prevention and management of diabetes. Additionally, Dr Raju is actively involved with the Global Association of Physicians of Indian Origin (GAPIO) and its US president Dr Sanku Rao. GAPIO represents about 1.2 million physicians of Indian origin, working in India and globally and focuses on improving healthcare standards.
Recent Comments